Condition
Hip Pain
Arthritis, dysplasia, labral tear, AVN, failed hip replacement
Hip pain can come from inside the joint, from the surrounding soft tissues, or referred from the spine. A clear diagnosis is the first step toward the right treatment — surgical or otherwise.
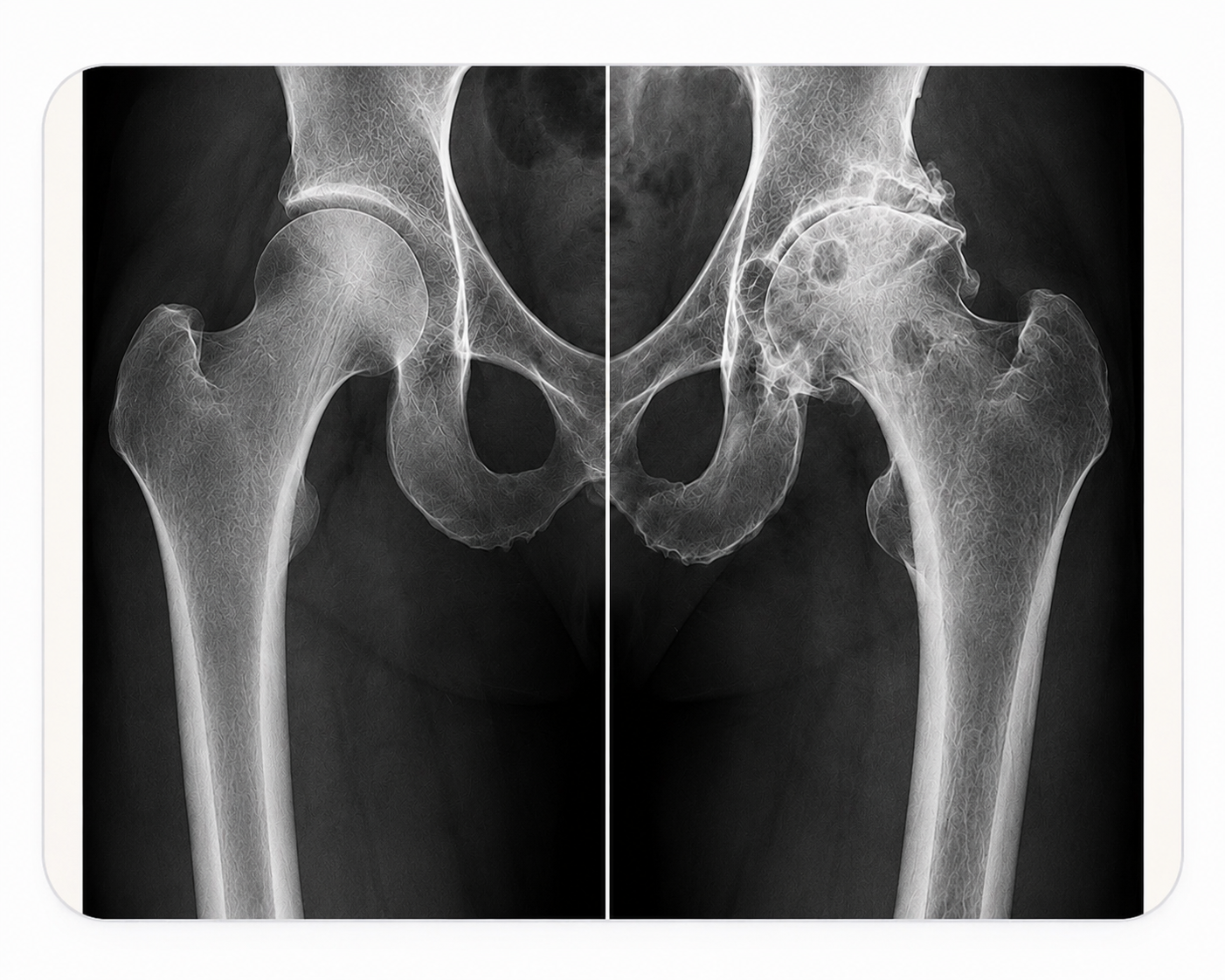 Normal HipArthritic Hip
Normal HipArthritic HipCauses of Hip Pain
Osteoarthritis
The most common cause of hip pain in adults — gradual wear of the cartilage lining the joint, leading to groin pain, stiffness and a progressive loss of movement.
Rheumatoid Arthritis
An inflammatory condition that can affect the hip joint at any age, causing pain, swelling and joint destruction that may ultimately require surgical intervention.
Labral Tears & Femoroacetabular Impingement (FAI)
Abnormal contact between the ball and socket of the hip, often seen in younger, active patients. Can cause groin pain, clicking and restricted movement, and may lead to early arthritis if left untreated.
Hip Dysplasia
A developmental condition where the hip socket is too shallow to fully cover the femoral head. It places abnormal stress on the joint and is a significant cause of early-onset arthritis in younger patients.
Trochanteric Bursitis & Gluteal Tendinopathy
Pain over the outer side of the hip, often aggravated by walking, climbing stairs or lying on the affected side.
Avascular Necrosis (AVN)
Loss of blood supply to the femoral head, causing the bone to collapse. Can occur spontaneously or as a consequence of previous conditions or treatments.
Previous Hip Conditions
A number of childhood and adolescent hip problems can lead to significant joint damage in adult life, including:
- Perthes disease — disruption to the blood supply of the femoral head during childhood, which can alter the shape of the joint permanently.
- Slipped upper capital femoral epiphysis (SUFE) — a displacement of the femoral head during adolescence, sometimes treated with fixation, which can subsequently lead to AVN, deformity or early arthritis.
- Rheumatoid arthritis presenting in younger patients.
Failed or Painful Hip Replacement
A previous hip replacement that has become painful, unstable or has stopped functioning as it should — whether due to loosening, infection, wear of the bearing surfaces, or instability — requires careful specialist assessment and may need revision surgery.
Investigations
Detailed clinical assessment of gait, range of movement and provocation tests to establish the source and nature of your symptoms.
X-ray of the pelvis, with ultrasound or MRI where soft tissue pathology, labral problems or underlying bone conditions need further clarification.
CT scan to assess rotational alignment, the relationship between the pelvis and hip, and complex deformity — particularly when planning a complex primary hip replacement or revision procedure.
Corin spinopelvic views where indicated, to assess spinopelvic balance and understand the dynamic relationship between the spine and pelvis — essential for guiding the optimal biomechanical positioning of a hip replacement.
Blood tests including inflammatory markers, and joint aspiration where infection or infection-related loosening is a possibility around an existing prosthesis.
Treatment Options
Conservative management
For most patients, the first step is always non-operative care:
- Activity modification, physiotherapy, targeted strengthening and weight management.
- Image-guided injections into the joint space, or aspiration of a painful or failing hip replacement, to confirm the diagnosis and provide relief.
- Hip arthroscopy for selected patients with femoroacetabular impingement or labral tears whose symptoms do not settle with injections and physiotherapy alone.
Surgical options
When surgery is required, the options range from straightforward to highly complex:
- Total hip replacement, including MAKO robotic-arm assisted surgery and the OPS (Optimised Positioning System) for precise, reproducible implant placement.
- Revision hip replacement, which may involve converting a previous hemiarthroplasty or hip resurfacing, revising a single component or bearing, or undertaking a full reconstruction of the acetabulum and femur where there is significant bone loss or deformity.